Subscriber Benefit
As a subscriber you can listen to articles at work, in the car, or while you work out. Subscribe Now
When Dr. Bill Tierney treats diabetics at Wishard Health Services, he has a huge range of medicines to choose from but little
actual evidence to help him choose.
That’s because the average drug has been tested in only 3,000 patients by the time it hits the market. If it proves
unsafe in fewer than 100 of those patients and in most of the rest produces a better effect than placebo sugar pills, it generally
gets approved.
“As a clinician, I really don’t care whether it works better than a placebo. I want to know if it works better
than metformin”—the standard, inexpensive drug to treat diabetes, said Tierney, who is chief of medicine at Wishard,
as well as a researcher at the Indiana University School of Medicine and the Regenstrief Institute. “There’s almost
no information out there about that.”
That’s about to change. The federal government is currently doling out $1.1 billion in stimulus funds to pay for research
that compares multiple medical treatments against one another to determine which is most effective.
 Wilkes
Wilkes
And beginning in 2013, so-called comparative-effectiveness research will get $500 million per year from dedicated taxes approved
in the new health reform law, according to estimates from the Brookings Institution.
Health insurance companies like Indianapolis-based WellPoint Inc. are eager to produce and use such research to make decisions
about what treatments to cover and how to price them.
But drug companies like Eli Lilly and Co., naturally, are wary that comparative-effectiveness research could threaten their
sales. The same could be true for some of the revenue sources of doctors, hospitals and medical-device companies.
Analysts view comparative-effectiveness research as a drag on revenue for health care companies, most notably drugmakers,
even though pharmaceuticals account for only 10 percent of health care spending. But there is a huge appetite on the part
of public and private health plans to pay higher prices only for new products and procedures that achieve major, not marginal,
improvements over existing treatments.
“There’s a concern that it will chill innovation in crowded areas where there are already existing therapies
present,” said David Johnson, CEO of BioCrossroads, an Indianapolis-based life sciences development group. He added,
“That’s a huge concern for all the companies that we work with, drugs and device.”
Kate Claessens, director of federal health policy and reimbursement for Roche Diagnostics’ U.S. unit, based in Indianapolis,
said the U.S. Health and Human Services Department has made drugs its top priority for comparative-effectiveness research.
Diagnostic devices, she predicted, probably won’t be affected for another several years.
Lilly already is making changes. It has been performing more clinical trials that pit its experimental drugs against existing
medicines, not just against placebos. And it has shifted its research and development into areas wide open for new discoveries—cancer,
Alzheimer’s and autoimmune diseases.
Lilly’s view is that comparative-effectiveness research can produce helpful information—as long as it’s
not used to really curtail anybody’s choices or reimbursement rates.
 “Comparative-effectiveness research may result in one-size-fits-all medicines,” Lilly
“Comparative-effectiveness research may result in one-size-fits-all medicines,” Lilly
spokesman Ed Sagebiel said in a statement. He added that any system the federal government sets up for using comparative-effectiveness
research “must ensure that the results from this type of research cannot be used to prevent patients from accessing
needed treatments, particularly vulnerable patients in government health programs like Medicare and Medicaid.”
The health reform law, signed by President Obama in March, bars the federal Medicare and Medicaid programs from using comparative-effectiveness
research as the sole basis for deciding how to reimburse for a particular medical product or procedure.
But WellPoint has the same policy and yet it has used comparative-effectiveness research, at times, to give less favorable
pricing to a drug.
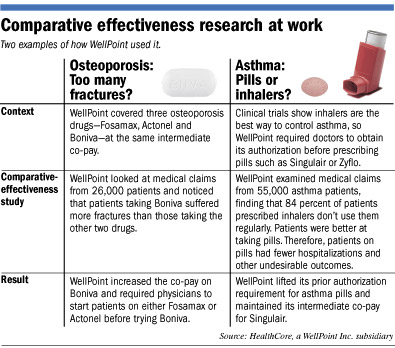
Just this year, WellPoint raised the co-pay on a prescription of the osteoporosis drug Boniva and required physicians to
try another similar drug before prescribing Boniva.
That decision came after WellPoint’s HealthCore subsidiary performed a study of 26,000 patients’ medical claims
and found that higher rates of Boniva patients suffered fractures compared with patients taking similar drugs Fosamax and
Actonel.
“Comparative effectiveness research is something that can help better value their product,” Brian Sweet, WellPoint’s
chief pharmacy officer, said of pharmaceutical companies. “If good science is done, and decision makers really use it,
it can really supplement what we’re getting from clinical trials.”
Not all of WellPoint’s decisions go against drug companies. For example, WellPoint’s HealthCore subsidiary performed
a study last year of medical claims from 55,000 patients with asthma.
Even though clinical trial data showed that inhalers were more effective than pills like Singulair at controlling asthma,
WellPoint’s study found that patients were far better at taking pills than using inhalers.
 Sweet
Sweet
Therefore, patients taking asthma pills had fewer emergency room visits and hospitalizations. So WellPoint decided against
raising its co-pay for Singulair and stopped requiring doctors to obtain prior authorization before prescribing it.
And sometimes comparative-effectiveness research yields no change from an insurer. In 2005, the New England Journal of
Medicine published a study of anti-psychotic drugs, including Lilly’s Zyprexa. On the whole, the study found, newer,
more expensive drugs were no better tolerated or more effective with patients than an older and much cheaper anti-psychotic.
But WellPoint made no change to its coverage policies after that study, in part because the study was only for patients with
schizophrenia, whereas the drugs are also commonly used in patients with bipolar disorder and depression.
So sales of the newer anti-psychotics just kept growing, leaping 43 percent over the next four years to nearly $15 billion,
according to IMS Health Inc., a market research company in Connecticut.
Tierney said such examples show that, until doctors are charged with keeping costs down, comparative-effectiveness research
won’t have a major impact on the nation’s $2.5 trillion annual health bill.
Comparative effectiveness studies “will change behavior,” he said. “And it’s not because of the evidence;
it’s because of the cost.”•
Please enable JavaScript to view this content.