Subscriber Benefit
As a subscriber you can listen to articles at work, in the car, or while you work out. Subscribe Now
Fishers Mayor Scott Fadness’ embrace of so-called “narrow” health insurance grew out of what had become an annual rite of frustration—the yearly spike in cost of coverage for employees and their dependents.
“What was happening year-in-year-out was that I would get in this room annually with these consultants, insurance brokers, all these different people, and they would tell me, ‘Hey, good news, Scott. This year, we think health insurance rates are only going to go up 8 to 12 to 13%,’” said Fadness, who became Fishers’ first mayor in 2015.

“I was thinking to myself, if that’s good news, I would hate to see a day when they said they have bad news.”
So Fishers made a big change, transitioning city employee health coverage to a narrow-network plan.
This year, Fishers employees have zero dollars deducted from their paychecks for health insurance premiums, and the city’s health care costs have been flat or decreased switching to a narrow-network exclusively in 2022.
But there’s a catch. Under the plan, Fishers employees must go to Community Health Network facilities for their care, with exceptions for travel or special cases.
The Fishers coverage is an example of a hospital direct-to-employer, or DTE, health insurance program. The city is contracting directly with Community Health for coverage, bypassing traditional health insurance plans such as those offered by Anthem Blue Cross and Blue Shield or UnitedHealthcare.
DTEs are called narrow plans because they restrict provider choice, but they are generally less expensive for employers and employees. Health insurers, including Anthem, also offer narrow-network options.
A state law passed this year means Hoosiers might see more narrow-network offerings as companies move into open enrollment season this fall. The law requires the largest hospitals to begin offering narrow-network plans this year and most other hospitals to offer the option in 2026.
Last year, the average cost of employer-sponsored health insurance for a U.S. family was $25,572, with the employee paying $6,296 of that, according to the Kaiser Family Foundation’s 2024 Employer Health Benefits Survey. The average premium for a single individual increased 6% from 2023 to 2024, and the average family premium increased 7%. That compares with an average 4.5% increase in workers’ wages over the same period.
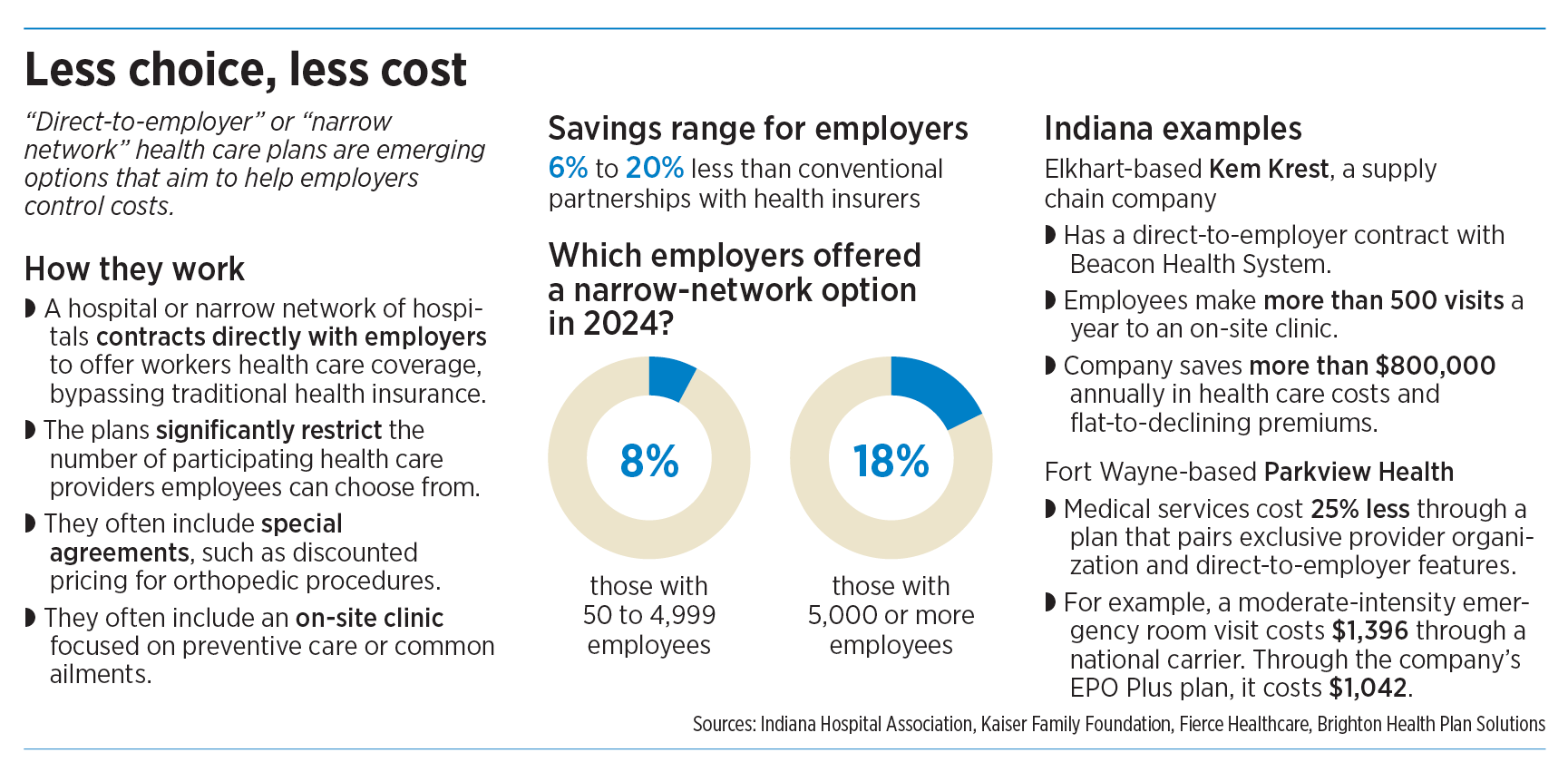
Industry experts say narrow networks, depending on the plan design, can cut those health care costs 20% or more.
In addition, hospitals say the direct arrangements also allow for flexibility in offerings as well as opportunities to better coordinate care, such as more quickly referring a patient from primary care to a specialist. Some DTE contacts are only for specific services, such as orthopedics.
Indianapolis-based Elevance Health’s Anthem Blue Cross and Blue Shield of Indiana, the state’s largest commercial health insurer, said direct-to-employer plans can be beneficial for some employers, especially those with workers concentrated in one geographic area.
“But we’ve found that DTE arrangements can be risky and potentially counterproductive for most employers,” Anthem spokesperson Jeff Blunt said in an email. “This is because health plans do much more than simply establish a payment rate with the local health system.”
He said employers have to consider the impact on workers living far from the contracting hospital system’s facilities and ensure compliance with changing state and federal regulations. In some cases, employers would also need to create behavior health networks.
“Employers would need to ensure that contracted hospitals can provide a comprehensive range of services to meet employees’ needs,” Blunt said. “This may include primary care, specialty services and emergency care, which can be challenging to consolidate within a single network.”
Anthem does not serve as a third-party administrator for DTE networks as it does for other health plans.
Additional benefits
Direct-to-employer and other narrow networks often include on-site clinics focused on preventive care or common ailments. They can include special agreements, such as discounted pricing for orthopedic procedures and agreements between hospital systems to broaden offerings or provide highly specialized care.

“The point … is to direct patients to where they can receive the highest-quality care at the best cost,” said Dr. Jason Row, a family physician and chief value transformation officer for Fort Wayne-based hospital system Parkview Health.
Parkview said it has more than 4,500 partnerships with employers, from organizations with two workers to those with more than 3,500, for an array of services such as employee clinics, specialty care and data analytics.
In April, Parkview introduced a narrow-network plan called Signature Care EPO Plus that it says costs about 25% less than commercial insurance networks.
Midsize hospitals also offer direct-to-employer and narrow-network coverage.
Hendricks Regional Health, based in Danville, has more than 600 direct contracts with employers, including with the town of Plainfield, whose employees receive services through the hospital system with an emphasis on primary care.
To serve those contracts, the hospital system has five Hendricks Regional Health Employer Wellness Center locations—four in Hendricks County and one in Indianapolis—for employees and their family members who are covered by its DTE plans. The centers offer preventive care and care for common health problems for no additional cost.

Gary Everling, chief strategy officer at Hendricks Regional Health, said the hospital system recommends to employers that they do not offer a narrow-network plan as the only option to their workers.
He pointed to challenges related to forcing workers to change what are often long-standing physician relationships because of a narrow network.
“That creates a lot of drama in the HR office and the CEO’s office,” he said.
Everling said the strategy is to give employees the freedom to choose their provider, with a caveat: “If I go wherever I want and it doesn’t include Hendricks, it might cost me a little bit more out of my pocket.”
New requirements
A new state law requires Indiana’s largest hospital systems—those with at least $2 billion in revenue in the state—to offer a direct-to-employer health plan with rates at or below 260% of Medicare reimbursement by Sept. 1 and most other general hospitals in the state to comply a year after that.
A recurring study updated in December by Los Angeles-based research group Rand Corp. found that Indiana hospital charges were 297% of Medicare reimbursement.
In part to battle those prices, narrow networks are becoming more popular with employers that are self-funded, meaning the company (rather than the insurance company) assumes the risk of employee health care and pays employees’ medical claims.
Health insurers offer their own narrow networks, including Anthem’s HealthSync, which it says cuts care costs 11% when compared with a traditional preferred provider organization, or PPO, plan. “It also adds a national network of high-performing providers to meet the needs of a distributed workforce,” Anthem’s Blunt said.
Fishers Mayor Fadness’ frustration drove him to talk with Community Health Network CEO Bryan Mills about ways to better control health coverage costs.
The result was a direct arrangement that launched as a pilot in 2019 between Fishers and Community, along with a third-party administrator to manage the program. The city initially offered employees the Community narrow-network coverage in addition to traditional insurance offerings. In 2022, the Community plan became the only option.
“We have not seen a single increase in health insurance,” Fadness said of the narrow-network plan with Community.
Fishers, a fast-growing Hamilton County city, offers health coverage to about 600 employees, including police officers, firefighters and other municipal workers. The number of people insured balloons to about 2,000, when covered family members are included.
The narrow choices have been no problem for Chad Hiner, a lieutenant with the Fishers Fire Department. He said he, his wife and children already used Community for their care and even under the narrow network, one family member was able to continue seeing a subspecialist physician in another hospital system.
Hiner said he especially appreciated Fishers working with Community to provide firefighters with what’s called the Galleri blood test by health care company Grail for early detection of multiple cancers. Occupational cancer is the leading cause of line-of-duty death in the fire service, according to the International Association of Fire Fighters labor union.

“It’s a very simple check to see what kind of markers are in the blood, and it’s a great thing for us,” Hiner said.
Dr. Patrick McGill, a family physician and chief transformation officer with Community, said the hospital system is looking to expand its narrow-network plan to other employers such as school districts and other cities.
“We’ve been able to show success with the city of Fishers, but other employers are a little hesitant to jump in,” he said. “You think of any other aspect of your life: If you want to lower costs, you have to restrict choice. I think that’s sometimes a very scary proposition for many employers.”
But McGill added: “What we’ve done is, we’ve really reduced a lot of the bureaucracy.”•
Please enable JavaScript to view this content.
Great article! There are two primary ways to control healthcare costs. The examples from Community, Hendricks, Hancock, Parkview, and others show the effectiveness of combining both strategies.
Because healthcare is a pay-for-service system, large insurance carriers traditionally use rationing as a strategy to lower costs. Rationing includes narrow networks, prior authorization, utilization review, formularies, and step therapy.
The other approach is to improve the health of the population. To state the obvious, this works because healthy people spend less on healthcare services.
What these hospital systems have done is use narrow networks to capture people within a system of care and focus on improving quality. The fact that their rates are lower and are not going up is proof that this can work.
There are ways that large insurance companies can compete by employing different strategies to improve population health; however, for now, hospital systems have the upper hand.